
Making it Count: Journey through Uganda in June
![]() Hannah Ikong
Hannah Ikong
![]() 16th June 2023
16th June 2023
How can we promote accessible and compassionate palliative care in Uganda?
Through a fundraiser walk? These days, counting each kilometre—or mile or step—can seem like a drudge of numerical exercise. Akin to a sitting room workout, we wonder on the point or reasoning behind so many push-ups every day.
I have participated in walks and other fundraisers before, but this year’s Journey through Uganda is more than the numbers completed. Actually, the journey is as much as a learning process on palliative care development as it is a reflection and a prayer.
You may have already started the milestone journey on our website. You’ll find that a cornerstone of the work in Uganda is education: training those who are working in health care and building capacity in our partner’s staff. Three of the Cairdeas scholars live in Uganda, with two advancing in social work while another completes studies in nursing.
We conducted a new interview with one scholar, Philip Amol Kuol, to hear his experience as a South Sudanese refugee, social worker, translator, and community health advocate. Philip recently told us, “Most of the patients are dying because of lack of good care to them. Because the more they realise that you are almost giving up on them, they feel like they should die … but if you have committed yourself to give good care to the person, the person will feel more that people still love them in the world.”
He shares more about the dignity and restored life given by access to quality palliative care below.
A recent pilot research conducted in the area where Philip Amol lives brings new perspective to the lived experiences of those with chronic illness. As we look through the Photovoice methods, from pictures taken and critical dialogue recorded, the reflection on Journey through Uganda continues.
In May, another scholar named Godfrey Oziti from Peace Hospice discussed his passion for palliative care with me. He defined his work as “a kind of care that gives the patient’s life back and is enjoying life again” and added: “I like to transform the patient so they are not just counting down the days.”
To cease the counting down of days to refocus on life again for a patient, I muse, as I think of how I count the kilometres for Journey through Uganda. Both involve numbers, yet I find joy in my counting exercise of this first-ever Cairdeas IPCT walk.
While I exercise and support the work of Cairdeas’ partners in Uganda, a chronically ill patient has just been treated and cared for with dignity and respect. As we build up the fundraiser more this June, more patients and their families find hope amid severe health-related suffering as trained health care professionals address physical, psychological, emotional, and spiritual concerns.
Our support during the Journey through Uganda funds those like Liz Nabirye, a Clinical Officer and Lead in the Palliative care Education and Research Consortium (PcERC). She not only offers consultations at no-cost to hospitalised patients but also trains dozens of medical students in palliative care.
I had the honour of attending a training with Liz Nabirye last week. When the question was asked on how to motivate a chronically ill patient to choose a healthy lifestyle and attend counselling, the rest of us were quiet and puzzled. Liz said, “There is a need to understand the circumstances which contribute to this person’s situation and identify what they think as a patient need to achieve. For example, there is need to be patient-centred and holistic in nature, which will definitely require multi-disciplinary support.”
The knowledge, skills, care, and approach being held by our partners Peace Hospice and PcERC have been spreading to their professional colleagues and medical students. Holistic palliative care is more accessible than ever before, and all at Cairdeas IPCT are pleased to be working with those in Uganda.
What an impact and how much value is being created for compassionate palliative care! Join us and register for the Journey through Uganda fundraiser this June.
Registration is open: from 15th April to 15th July this summer!

A leafy hillside road in Kampala, Uganda: a great place for reflection.

Toko Friday Santiago (left) stands with Philip Amol Kuol (middle) and Dr Mhoira Leng.

Godfrey Oziti during training of village health teams (VHTs).
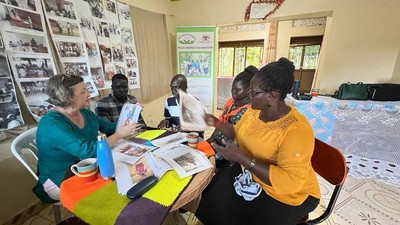
Dr Mhoira Leng leads an initial analysis on Photovoice pilot research with (left to right) Simon Maku, Toko Friday Santiago, Immaculate Atim, and Vicky Opia.

Liz Nabirye (right) walks alongside Jennie Twesige (left) to Mulago Hospital, Kampala.
Engage in the journey with us; after registering you can join our WhatsApp group!
Granted Dignity and Humanity: Experience of Palliative Care in Gaza
![]() Hannah Ikong
Hannah Ikong
![]() 14th June 2023
14th June 2023
In the last year, Cairdeas IPCT has partnered with the Islamic University of Gaza (IUG) and the Turkish-Palestinian Friendship Hospital (TPFH) to create a palliative care professional diploma programme. Together, with the support of the University of Edinburgh and Palliative Care in Humanitarian Aid Situations and Emergencies (PallCHASE), the students have covered six modules of instruction with visiting faculty, as well as clinical instruction and fortnightly, virtual teaching sessions.
Our Medical Director, Dr Mhoira Leng, alongside Dr Khamis Elessi the Gaza lead, have been mentoring and supporting the TPFH to develop and implement a palliative care clinical programme.
The next international faculty visits will be in August 2023, and we wanted to hear from some of the students for their key observations, feedback, and experiences. We asked members of the TPFH palliative care team who are also students on the Diploma.
One student, Suha S. Shaa’th, a senior pharmacist who is also the lead for opiate procurement, shared several reflections on palliative care. She explained “the importance of letting patients live in dignity and die in peace,” while adding that “palliative care reinforces the sense of humanity and improve the concept of compassion and empathy, that means we do not deal with patients as numbers.” Suha highlighted her skills gained through the diploma programme, such as communication, working in multidisciplinary teams and evidence-based practice.
A physician specialising in pain and palliative care management at TPFH, Amjad F. Eleiwa, spoke about the knowledge gained from the programme, saying, “I started to deal with the patient not only as someone in pain, but also as a whole person.” Amjad then shared a patient story to illustrate holistic care:
"A few weeks back, I had a 26-year-old patient who was diagnosed to have Ewing sarcoma. The patient started his management in Jordan then was referred back to Gaza after expiring all lines of treatment … The issue we faced is the shortage of controlled release oral morphine in Gaza and that is where the palliative care training came in. We started to look for available alternatives and gave him sub cutaneous injections of morphine and patches of fentanyl. His pain started to get under control."
"During our work with the patient, we noticed that he accepted his condition but not his mother. She was so close to him and she had a lot of questions like "why him?". We had our focus on the patient and on his mother to prepare her for the inevitable: his death."
"At the end, she was thankful that he died in peace with no pain and with great acceptance."
We will close with the comments from Basel M. Ashour, a psychologist and student in the diploma programme. Basel noted that “psychological pain is considered one of the most aggressive pain among cancer patients” then discussed how “palliative care added to my experience how to know other team’s knowledge … about nutrition, pain management, physiotherapy, etc.”
He concluded: “Many people just need us to spend time with them, to communicate well, to be dealt with extra respect and be granted dignity and humanity.”
We will share more of the experiences of students and faculty in the future. We thank all the students in diploma programme for their implantation of compassionate palliative care; may we all continue to uphold dignity and humanity.

Students gather to watch the virtual presentation during a teaching session.

In this teaching session, Dr Khamis Elessi is in person, while Dr Mhoira Leng and Dr Nahla Gafer connect over Zoom.

Suha S. Shaa’th, Mervat Abdelkarim Hammad and Nour M Almasry during a ward round as they discuss the patient.

Psychologist Basel M Ashour with a patient on a ward round.

Multidisciplinary team work among students and their colleagues.
An interview with Godfrey Oziti, Cairdeas Scholar
![]() Hannah Ikong
Hannah Ikong
![]() 30th May 2023
30th May 2023
Godfrey Oziti may be a name you’ve heard of before in Cairdeas IPCT. Godfrey serves as a nurse with our partner Peace Hospice in Adjumani and Obongi districts (Northern Uganda), is involved in many training and research activities, and now is a Cairdeas Scholar as he continues his education in nursing.
You may have also met Godfrey in our March 2020 blog on palliative care services during COVID-19 in Northern Uganda. Rereading this blog and speaking to Godfrey more over this last month has brought me to a realisation: Godfrey has a huge heart for his patients.
In our last conversation, I asked him to define “palliative care.” I am always curious of how those have worked or specialised in a field for some time put “palliative care” in their own words. Godfrey didn’t tell me a textbook definition either; rather, he captured the heart of palliative medicine by telling me a story.
“Let me start with a scenario. Okay, once I paid a visit to a certain patient in the community and the patient had a fungating wound that was smelling really bad. The family was locking the patient inside a room because they said that he was smelling badly. At first the family first refused me to come in there. But I insisted and then I went inside with the patient. I asked them to bring soap and water, and then I bathed him and arranged the room. After that, I told them to bring them food and we started with tea, and we kept on eating. And he [the patient] was very happy to be staying in a clean environment and eating.”
Godfrey went on to explain the symptom management of the wound, how they could help with the patient’s pain, and what he did to work with the family to understand the patient’s condition and how to care for the patient well.
After talking about this particular patient, he begin to tell me that there is indeed a need for community sensitisation and education on palliative care needs. “We do love our families” he explained, “but sometimes with they are sick, we leave them alone. And so the psychological diseases take many of our patients. And there is really a need for us and with my studies, I know we should do more.”
His studies! I had to ask about the scholarship that he received and how school was going. He started his Diploma in nursing this year and will be going for the first end of semester exams soon. The programme is a year and a half, located in the Gulu School of Nursing and Midwifery.
Asking about his schooling quickly turned to plans of the future. “I know that from here, I can do any other course or diploma,” Godfrey explained after saying that it was his dream to go back to school. “Our medical nursing tutor is very encouraging and gives us career guidance so I am really learning so much from her. She elaborates on what to do and how to go to the next step in their career. She adds this advice to her lectures.”
He’s looking forward to the next semester already as one of the courses is an introduction to medical research, including its theories and principles. Godfrey was quick to tell me that he really has enjoyed his time in data collection in the several research projects involving Cairdeas IPCT and Peace Hospice.
He was also quick to explain why: “I love talking to the participants and getting their views, how they are really coping up with their challenges and how we are addressing them. That’s what I really enjoy, getting to know someone’s problem and then and then offering psychosocial support afterwards too.”
I wanted to dig a little deeper; to better understand Godfrey’s heart for patients and how he has learned this approach. When I asked about professional mentors in nursing or palliative, the name “Vicky Opia” appeared, the Peace Hospice Executive Director and Palliative Care Ministry of Health lead for Adjumani district. This is what he told me:
“Sister Vicky has mentored me mostly in palliative care because in my [nursing] certificate, there was only a small part of the course in palliative care. When I join Peace Hospice, the first thing I noticed was how she handled patients with chronic illnesses and the way she did her work; how she was giving care to the patients was inspiring. So I started to copy what she was doing and how she was relating with the patients. I thought to myself, I need to start working with chronic illnesses. I need to work like Sister Vicky. Even if I do not go back to school, I need to work like Sister Vicky. That is how I started to love my work so much.”
Godfrey then explained how at the beginning, he met a patient in critical condition who had given up on life. “The nursing care that was modelled for me by Sister Vicky was a kind of care that gives the patient’s life back and is enjoying life again. I like to transform the patient’s life, so they are not just counting down the days.”
As a Cairdeas Scholar and nurse at Peace Hospice, Godfrey is looking forward to doing more palliative care work in his future. He hopes to keep on studying (or learning) and is most concerned working with refugees and other vulnerable populations.
Godfrey is concerned that there is not enough of the right type of health care worker to provide for palliative care. “You know,” he told me in closing, “the people available with the knowledge of palliative care and with the time to talk to the patient and family members are not there. But if I can go through my studies and go through to be a specialist, then I can do more as Peace Hospice is concerned.”
His heart for the patient – compassionate, quality palliative care service provision at its best – as well as his concern for patients without such services is a call to action at Cairdeas. We must continue the capacity building, training, advocacy and research to support palliative care services with health care systems as well as for communities and individuals.
As an individual, Godfrey’s last comment was one of gratitude, thanking Cairdeas for the partnership and support of Peace Hospice. “I am so happy for Cairdeas for carrying out the different training for village health teams (VHTs) and health care workers and providing scholarships for people like me. I hope they continue to expand the scholarship programme.”

Godfrey Oziti in the Peace Hospice uniform, giving feedback during a recent training.

Godfrey Oziti (left) sits on the ferry crossing the Nile River next to Dr Mhoira Leng and Simon Maku.
Godfrey Oziti leads a discussion on community generated research data with village health teams in Obongi district.

A snap from Godfrey himself.