
BlogBe notified of new blogs
Walking Two Paths with One Heart: An Interview with Liz Nabirye
![]() Cameron Don
Cameron Don
![]() 10th July 2026
10th July 2026
One of the key areas of work Cairdeas has been investing in over the past few years is our scholarship programme in Uganda, through which we have been building up local palliative care leaders for the future. It is a key pillar of our committment to facilitating locally-led development of palliative care in Uganda, and we thank our supporters for helping to fund this programme as part of our ongoing work.
One of these scholars is Elizabeth Nabirye, who is coming to the end of her time as a Cairdeas scholar, studying for her Master’s Degree in Palliative Care. Elizabeth, or Liz as we know her, also works as the Clinical Lead at PcERC, our partner in Uganda. Recently I sat down with Liz, via Zoom, to discuss her time as a Cairdeas scholar and leader at PcERC, her research and insights from working with rural communities, her plans for the future and her exciting new life as a grandmother.
Hi Liz, thank you for taking the time to speak with me today. Our supporters will know that you are one of our Cairdeas scholars, currently studying for a master’s degree. Could you tell us a bit more about the work you’ve been doing, the research, and your experience of being a Cairdeas scholar.
Yes, thank you so much for the opportunity!
I'm called Elizabeth Nabirye and I'm the clinical lead of PcERC, which is the Palliative Care Education & Research Consortium and currently I am finishing up my Master's degree in Palliative Care. I'm glad I got the opportunity to be one of the scholars of Cairdeas and this gave me an opportunity to embark on this insightful and rewarding program. Even when I've spent more than 20 years doing palliative care, there's been a lot to learn from the program. It gave me an opportunity because already I have a bachelor's degree in palliative care and did a nurse prescribing diploma.
One of my specialties during this course has been the paediatric palliative care. There's a lot more to children than just what we think. And so with this scholarship, it gave me an opportunity to learn more about children. It gave me something to think of as a student, as a scholar. What about pediatric palliative care; who is providing it in our country, Uganda, and what needs to be done? I had a lot of questions about children because I'm passionate about them, as a mother, and now also as a grandmother. One of them [my children] struggles with a life limiting condition. So I appreciate and I know what that means for a mother but also for the children.
So when it came to choosing my topic, on what I can study to add value to the clinical practice or to policy, I thought of children. My studies are looking at the nurse prescribers or clinical officers who are in Uganda, who are working at regional referral hospitals, what is their experience [with children], who knows about them? Because the course that is done about prescribing is mostly inclined towards adults, most of the teaching is about adult palliative care. But when you go out to the field or go out to the communities, you become the consultant there and you are expected to be seeing & taking care of not just the adults, but also the children.
And in my experience, as I thought about them, I developed my proposal, got an EDCA approval, and I've been collecting data. It's been amazing to hear from these nurse prescribers in Uganda who are working in the regional referral hospitals. Regional referral hospitals are the big hubs, where complex conditions are referred to from the community, from the district or general hospitals before they get to a national referral hospital where I'm working. And what I've heard from them made me realise that, wow this is interesting, because there's a lot to add on knowledge and also maybe to inform policy in terms of different things that I found out in my study.
So currently, I'm done with collecting data. I interviewed 20 participants from 13 regional referral hospitals across the country. I've been collecting data using recorded interviews, telephone recorded interviews. And initially I didn't think it was feasible, but it's amazing to know how innovation and limited resources can produce good outcomes.
Thank you. That's great to hear. One thing I wanted to ask about was, you've previously spoken about evidence in palliative care extending beyond just the statistics and into the powerful stories of patients and professionals. Can you tell us some more about that?
So yes, the stories are many and palliative care is, just like you put it, beyond the numbers that we see. Beyond each of the statistics, there are lots of stories and most of the times they are challenging stories and this is what keeps us going as palliative care providers.
For example, I'm a mother to a child with a life-limiting condition and because of that, I get sometimes taken up or swallowed up by the emotions when every day I have to listen to parents, mothers or fathers or grandparents struggling with children living with life-limiting conditions. And it can be complex, especially in a limited resource setting.
There's complexity where there is stigma, you find a mother struggling with the child and has been abandoned by the family or the husband, just because this child has a life-limiting condition, or you find some parent has travelled from upcountry, and no one can talk to them because of a language problem.
In Uganda, we get many refugees. Sometimes you find they are by themselves, and even just being there to listen to their story, maybe that's what the best you can do. But sometimes you feel your hands are tied, given their needs, and you can't fulfill all of them.
And sometimes it can be draining, but it can be rewarding; you appreciate the meaning of life, but also you appreciate what people go through. And personally, I would say this kind of exposure, this kind of interface with people who are struggling with life-limiting conditions, whether adults or children, has strengthened my spirituality, has grown my spirituality to know that all these are made in God's image.
But because of our system challenges, you find there's a lot of inequality in terms of services, in terms of what people can achieve. And all this teaches me that every patient, every person is unique in their own ways, even when they have a similar or the same diagnosis.
Even when someone is losing their loved ones, I've appreciated or I've gotten a fulfillment when I hear someone, who lost their loved one, but they benefited from my services and or from the palliative care services and they appreciate even after the loss. Sometimes patients leave the hospital and die from home and then the family call you just to inform you that ‘my mother passed on but thank you so much.’ That alone keeps me going.
And if you can, would you be able to share with us one of those stories that's really shaped you or shaped your perspective over the years?
One particular case that really touched me was a case of a mother who I met with a child who was struggling with HIV and cancer, and the child was in a lot of pain.
This child had just lost a dad, and the mother had another two children, but the family had abandoned them because one, they were HIV positive, the child and the mother, but two, he again got cancer, so it was a bit complex.
After managing his pain, we asked this child if there were any questions he wanted to ask. And we were amazed by his questions, it was an eye-opener when it comes to communicating with children.
One of the questions that this child asked was, if it is painful when people die, whether it hurts when you're dead. And then he also asked, where do people go when they die?
This was a nine-year-old, but because of the illness, it seemed like a three or four years old. So when asked about whether it's painful, the obvious answer of me as a health care worker or as a care provider is the quick way of saying it is not painful.
And again, he asked about ‘where do people go?’ And the obvious answer is that the teaching from Sunday school, if you're a Christian, is that people go to heaven when they die.
And then he asked another question, whether his mother would be hurt when he dies? And the obvious answer was that, of course, when people lose their loved ones, they feel bad, they get hurt, they feel pain.
And then this child shook his head and said, “You're lying.”
And for me that was like, ‘excuse me, what do you mean by we are lying?’ And he said, “Are you sure when people die they go to heaven?”
And he just shared his experience. He said in his small voice, low tone, that when he lost his dad, their dad was wrapped in a cloth, and then they dug a pit and they lowered him there, and poured in soil and stones.
So, that had two folds. One: is the way to heaven underground? Because his father was buried in a grave and they keep telling him that the father went to heaven. But also his imagination is that if you're hurting now and then you die and they put you in a pit or grave, and they pour on soil or stones, it must be painful. And with that, his request was, when I die, can you buy for me a metallic box?
So for me, that was one thing that just opened my mind when it comes to communicating with children.
The other question was when he asked if the mother would be hurt [when he died] and he didn't think so because most of the times his mother keeps telling him ‘you're not dying, you're not getting better and I'm struggling. I've struggled to buy this expensive medicine and you vomited it, I've given you food and you refused to eat.’ So to him that meant that the mother will celebrate when he died.
And so what this story taught me as a clinician, it taught me that we just need to know the language, know what the question is about that our patients are asking, because we got it all wrong.
Sometimes patients ask us, am I going to die? And we are quick saying, no, we are doing our best, but when actually they are going to die or they just want information to plan, to make decisions about whether they should take the patient home and we fear to open up and talk about prognosis.
Human beings are individuals, and what that child asks, maybe it would be different from the needs of another child. So what I learned from this case, what stuck in my memory is, ‘when people ask us questions, why are they asking us? What exactly do they want?’
Well, thank you very much for sharing that. That story certainly highlights that we do learn as much from the mistakes or when we get things wrong as we do from the teaching and the successes as well.
And then also reflecting on your studies, I know you've spoken about wanting to publish findings that highlight rural perspectives on paediatric palliative care. Could you just tell us a little bit about your experience working alongside rural communities and the particular challenges that they face?
One of the things, the biggest challenge, is the resource limitation. And you find, especially when it comes to children, these are minors and the decisions are made on their behalf. When they get sick, it's not them to decide whether they should come to hospital or not. They are dependent on adults. In the community, there are many needs. There are many issues. One of them is their beliefs. You find there are a lot of beliefs in the community or society about illness and about death.
So you find when someone has a life-limiting condition, whether malignant or neurological, things like epilepsy or cardiac issues, you find that the first thinking of the parents or the community is traditional medicine or witchcraft. So that alone delays access, or delays people seeking medical intervention or seeking medical help and making it worse.
The limited resources you find that in that community, the nearest health facility could be maybe 20 kilometers. But the traditional healers or the witch doctors, they're easily accessible. So most of the time, those are the first people that the sick will go to, whether a child or adult. Because of the distances they have to travel, and when they do get to those facilities, there is a limited resource in terms of human staffing and so sometimes they have to move around a hundred kilometers to get to somewhere where they're going to get a clinical officer or a medical officer who is going to do a proper assessment and get them treatment.
So whether before diagnosis or even after diagnosis, you find that working in a community is emotionally draining because sometimes even when you know what you're supposed to do for the patient, you cannot do it.
For example, currently I work in Mulago, and I'm called to see a patient and then I assess them and do end of life care counseling and ask them whether maybe home would be the best place, and they can decide they would want to go home.
But they're going into the community where they cannot even access morphine, for example. And even when they are dying, they have the right to pain control, but they can't access that. Also because of the fact that the family or the community knows they are dying, sometimes they don't think they need care, in quotes, I would say they call it wasting.
And because most of the palliative care trained specialists are in the hospitals, or they are not in the community, or they cannot even afford to do home-based care. So you find a patient whose symptoms were managed or controlled in the hospital, they die [in the community] without dignity, with a lot of suffering.
And this impacts on not just the patient, but also the family. Because sometimes I get phone calls where they will say, the morphine got finished, for example, and we couldn't access it anywhere, and they wouldn't travel back. But also, their only wish or prayer was that they were glad that their loved one died, because that was the only way to relieve their suffering. And to me, that is terrible, I would say.
For example, when it comes to the roads, sometimes I've had to counsel families to allow the patient to die in an urban or hospital setting. Just because of their condition and how they're going to travel on the roads. Everyone doesn't own a car in Uganda and a patient cannot sit on a bike, but their home is not easily accessible.
There's a lot to be done, not just by the palliative care specialist, but there are system challenges. I mean, we need a lot of things where someone will have a choice of where they want to be cared for or where they want to die from and die with dignity and they get all that they need.
Because sometimes people have had to travel many kilometers from their community to the hospital to emergency department. Not because they expect miracles, but because they can no longer just watch their loved ones there. So even when they know they are dying, if they love them, they'll still rush to hospitals, so the patient dies where maybe they'll be able to get symptom management.
Yes, those are some really difficult challenges for those communities. And thank you again for sharing.
So we've spoken a bit about your experience as a scholar and your studies, but also, you work as a clinical lead for PcERC. Could you share with us where these two paths have met, where the scholar and the practitioner paths have linked together and how they impact on each other?
Like I mentioned before, going back to school to do this masters as a Cairdeas scholar was exciting and was a way of developing not just my professional development, but also personally.
And as a leader, there is a lot of learning. There's a lot of teaching about leadership, because at this level, it's not just about the clinical care, but other things that are taught there.
So one good thing about being both a clinical lead and also a scholar is that I'm involved, I'm placed in a clinical setting and some people don't have that privilege. They have to go from their workplace to a different place, to get the practical experience. So I've been lucky that what I learn, I can practice.
And also, I'm able to pass on the knowledge, and also to see things in a reality. What has been taught, or what I've been able to learn. I've learned that, for example, I can give an example of being a clinical lead, and also being a scholar.
So even when it comes to resources, like appreciating or delegating, I'm able to say as a lead, maybe like when I was requesting for my study day or my time, is to know that the work will be done, can I learn to delegate, can someone else do what I'm supposed to do?
But in the process, because you are both a student and also a leader, then by default you have to learn certain things. And with that, then I can talk about what does it mean being a leader and being a student? So to me, it's rewarding, but also demanding, I can say.
And it's rewarding, especially when you're putting what you're learning in practice and when you see value and relevancy of the competences you're acquiring.
That's great. Thank you very much. So, your studies are nearing completion, I think you're finishing in in August this year.
What is it you're looking forward to or most excited about as you move on to the next stage of your learning or your career in palliative care?
One thing I've noted about palliative care is that everywhere there's need for training. And I think after my masters, I need to be thinking whether I can do a PhD or a fellowship, because there's still a big knowledge gap.
So one of the things is like, how do we pass on the knowledge that we have? Because that is the way to sustain palliative care, to educate and train.
Even when you're teaching, yes we need to teach basic palliative care, but also advanced palliative care so that people are able to advocate. And also, we need to keep that confidence of being able to inform at a policy level.
The other thing is that we need evidence. This study that I've just done, when you go to literature search, you'll find there's a lot of information. But is it in the context? Is it local evidence?
So there's a lot to prove to the people we are advocating to, the policy makers, that this is here with us and these are the facts. We need to do more research or do things that really relate to our settings, especially resource limited settings, because there's a lot of literature, there's a lot of research on what has been done in developed countries, and unfortunately, it's not a copy and paste. And policymakers need evidence that is local, and specific to the needs of the local area.
Yes. Well, that's great. We’re excited to see where you go next. A PhD sounds like an exciting plan!
Thank you for sharing all of this with us Liz. I just wanted to finish on this, we know that you've recently become a grandmother for the first time with two new grandchildren! How are you enjoying that and how are you adjusting to life as a grandmother?
Yeah, it's exciting because I used to see my own grandmother as very old!
It was exciting, first of all, seeing the children, they've been babies and most of the palliative care fraternity know about my children. I joined the palliative care when they were still small and they've seen them grow.
And it's been amazing just to know that my son is married and has a baby. Of course, it comes with all its demands because when, like, for example, my daughter-in-law was big, was expecting, there were a lot of things that come with pregnancy and when they came to that time of delivering the first grandchild, she had had to be delivered before term.
And then when I came in as a mother, but also as a counselor, because there were many questions. What does it mean having a seizure? What does it mean to become weak?
And there was a lot of allaying anxiety and giving information because my son, he chose to go with the wife to theatre. So I first had to explain to her what to expect, to him what to expect. And for him, he just felt he needed to be there with his wife to support. But then eventually he collapsed while in theatre.
Oh, really?
I know. (laughing) During the c-section.
But the good news for me, what I appreciate, was how supportive he was to his wife, but also the fact that he got all the information that he needed before he made that decision.
And yeah, so it was a bit excited because I've been in school, I've been a lead and then I have two expectant mothers that really are close to me. I don't call my daughter-in-law a daughter-in-law, I call her a daughter-in-love. And I don't even think of laws because I've told them it's not about law. It's interesting because when people come to marry, they ask to be part of the family. They should be children in the family. So I'm like a mother of twins.
The first set is the son and the wife, and the second set is my daughter and the husband. And now both of them, they are pregnant, one following the other. It’s one of these things that you look forward to, but now you also think, as I graduate, these small babies, what will they be?
My colleagues were with me in the hospital when my daughter had just delivered. It was delivered from a near hospital. It's not just about me, it's about the whole palliative care fraternity. They attended like my daughter's function, marriage function, wedding.
So being a jajja (Ugandan term for Grandparent) is like someone who, it is expected that you should be now taking care of the grandchildren. But you are in school, and you also think of being a lead, so I've had three major things that I just did not compromise. I think a jajja is a given, but yeah, I also have those other responsibilities.
So it is interesting because even when I'm taking care of the grandchildren, when they visit me, I have to put aside everything, whether academic, but also my team has been understanding. Like now I have, if I left early, then they would know this is the jajja is going to attend the grandchild.
And children are small angels. And I'm passionate about children. It's been timely because my boy and girl, they would tell me, you are the pain specialist, and can we give morphine, of course, making a joke, making a big joke of me. (laughing)
Of course, these are my children. I look at you and say, wow, it's been a journey. And now here we are.
Well, that's amazing, Liz. Thank you very much for sharing everything today and taking the time to speak with me, I really appreciate it.
Thank you, it's been a pleasure.
We would like to thank Liz again for taking time out from her busy schedule of studies, work and helping with grandchildren to speak to us. We want to continue helping to build up palliative care leaders like Liz, to continue to invest in palliative care in Uganda and help to solve some of those challenges spoken about.
We can only do this through support from donors, who allow us to fund scholarships and invest in the in-country leaders who can advocate for locally-led, sustainable palliative care. Please consider starting or increasing your donation, which you can do by following the link below, thank you.

Liz Nabirye (pictured right) is one of our scholars, graduating in August this year!


The team working with a child patient, including another Cairdeas scholar, Toko Friday Santiago (pictured middle)

Members of the Palliative Care Education and Research Consortium (PcERC)

"Children are small angels"

Jajja Liz meeting her grandchild
‘My Experience Creating and Presenting a Poster at the African Palliative Care Conference in Gaborone, Botswana’ - Toko Friday Santiago
![]() Cameron Don
Cameron Don
![]() 9th April 2026
9th April 2026
One of our graduate scholars, Toko Friday Santiago, travelled to Botswana in September for the African Palliative Care Conference, presenting some of his research work on social protection issues for refugees. We were delighted to sponsor this opportunity for Toko and current Cairdeas scholar, Phillip Amol Kuol, who both hold such great passion and desire to give back to their communities. I asked Toko to share his experience of the conference and sharing his research, and how opportunities like these help with his continued professional development.
In September, I had the privilege of attending and presenting a poster at the African Palliative Care Conference held in Gaborone, Botswana. The conference brought together healthcare professionals, researchers, policymakers, and advocates from across Africa and beyond to share knowledge and innovations aimed at improving palliative care services. For me, this experience marked an important milestone in my academic and professional journey as an emerging researcher interested in issues of vulnerability, health equity, and social protection.
My poster focused on exploring the factors that promote social protection among the refugees in Palorinya Refugee settlement. Refugees often face numerous challenges including poverty, trauma, limited access to healthcare services, and social exclusion. In such circumstances, social protection mechanisms such as community support, humanitarian assistance, and inclusive health programs play a crucial role in addressing both the health and social needs of these vulnerable populations.
Preparing the poster was an exciting and challenging process. Translating research ideas into a concise visual format required careful thought and creativity. A poster presentation must communicate key findings clearly and quickly, often to audiences from different professional backgrounds. I had to think critically about what information was most important and how best to present it in a way that could spark discussion and interest among conference participants.
Designing the poster also pushed me to develop new communication skills, learning how to balance text, visuals, and data so that the message remained clear, engaging, and accessible to a diverse audience. This experience helped me appreciate the importance of communicating research in ways that are both informative and visually appealing.
The poster session was one of the most memorable parts of the conference. Researchers, clinicians, and policymakers walked through the exhibition area, stopping to engage with presenters and discuss their work. Standing beside my poster, I had the opportunity to share the motivation behind the research and explain why social protection is critical for refugee populations.
Many participants expressed interest in the topic and shared their own experiences working with displaced communities in different parts of Africa. These conversations were particularly meaningful because they highlighted how the challenges faced by refugees are shared across many contexts on the continent.
The discussions that followed were incredibly enriching. Participants asked thoughtful questions, shared insights from their own work, and reflected on how similar approaches could be applied in other settings. These conversations highlighted the growing recognition of the need to address social determinants of health within palliative care.
Presenting at the conference was a deeply rewarding experience. It challenged me to step outside my comfort zone and engage with an international audience of experts and practitioners. Interacting with professionals from different countries and disciplines broadened my perspective and reinforced the importance of collaboration in addressing complex health and humanitarian challenges.
One of the most important lessons I learned was the value of dialogue and knowledge exchange. Conferences such as the African Palliative Care Conference create opportunities for professionals from diverse disciplines and regions to learn from one another. Through these exchanges, new ideas emerge and innovative solutions to complex health challenges can be developed.
The experience also strengthened my confidence as an emerging researcher. Sharing my work on such a platform affirmed the importance of research that highlights the needs of marginalized communities, particularly refugees who often remain underrepresented in health discussions.
Participating in the conference has inspired me to continue exploring ways to strengthen palliative care services for vulnerable populations. There is a growing need to integrate social protection, community support systems, and culturally sensitive care approaches into health programs that serve displaced communities.
As Africa continues to face humanitarian challenges and population displacement, it is essential that health systems and social services work together to ensure that no one is left behind.
I am deeply grateful to organizations such as Cairdeas International Palliative Care Trust that supported my participation in the conference. Opportunities like this not only contribute to professional development but also help amplify important conversations about health equity, dignity, and compassionate care for vulnerable populations.
Attending and presenting at the African Palliative Care Conference in Gaborone was an unforgettable experience. It reminded me that research is not only about generating knowledge it is also about advocating for change and giving voice to communities whose stories deserve to be heard.
Thank you to Toko for sharing your experiences at the APCA conference, and for the wonderful work you do helping refugee populations. We are excited to see your work continue and grow, making a difference to those who need it most, and promoting the expansion of palliative care in Africa.

APCA 2025: Gaborone, Botswana
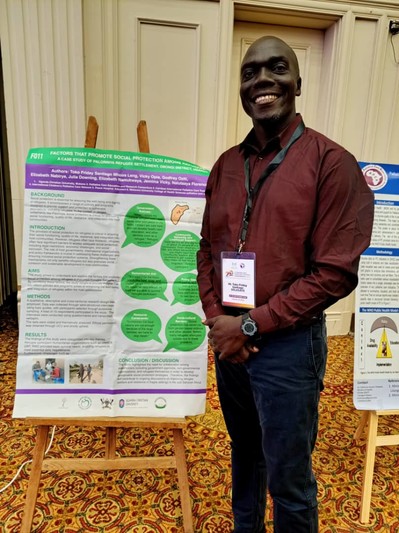
Toko with his research poster
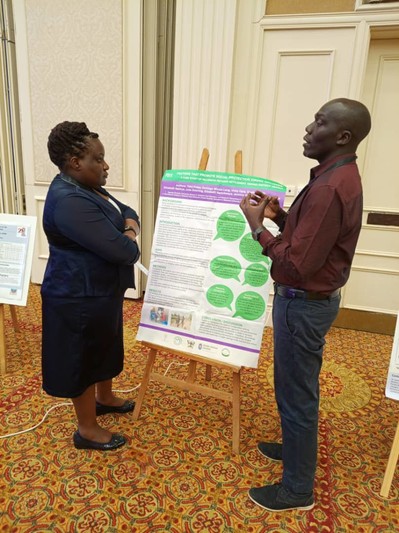
Toko discusses his research with a colleague
The Cairdeas team at APCA 2025
Conference Report - ‘Palliative Care: rethinking coping, exploring hope, in the midst of conflict and change.’ by Michelle McGannan
![]() Cameron Don
Cameron Don
![]() 26th March 2026
26th March 2026
In February, Cairdeas joined with Ednburgh University's Global Health Academy & PallCHASE (Palliative Care in Humanitarian Aid Situations and Emergencies) to host a hybrid conference, entitled 'Palliative Care: rethinking coping, exploring hope, in the midst of conflict and change.' This conference was a wonderful time of community among the global movement to make palliative care accessible to all, and we were delighted to help bring together so many friends and colleagues from over the years, to discuss this most pressing global health challenge.
Michelle McGannan, one of the conference's organising committee members and a member of PallCHASE, wrote this report on the conference for the e-hospice and kindly agreed to share it with us, so we could bring some of the content from the conference to our supporters.
The Global Health Academy (GHA) at University of Edinburgh, PallCHASE (Palliative Care in Humanitarian Aid Situations and Emergencies) and Cairdeas International Palliative Care Trust were delighted to jointly undertake this hybrid conference. We were joined by 26 participants in-person in Edinburgh, Scotland, and 43 online from countries including South Africa, Lesotho, Malaysia, Mozambique, Jordan, Kenya, Ghana, Ukraine, Germany, Dubai and Egypt.
The conference began with a welcome by Prof Liz Grant (Scotland), where the importance of compassion in both responding to, and taking action to alleviate, suffering was emphasised, with participants being challenged to consider what action can be undertaken individually and collectively.
The plenary sessions commenced with Dr Mhoira Leng (Scotland, Gaza and Uganda) setting the context of palliative care in humanitarian crises/conflict settings, including a focus on non-communicable diseases and holistic needs, with an emphasis on the need to hold onto our shared humanity. Practice exemplars from Sudan and northern Uganda were shared, emphasising the importance of the emerging evidence base. The 2024 WHO report ‘In the Line of Fire’ which outlines the ever-increasing attacks on healthcare workers in conflict zones including Gaza, Ukraine and Myanmar, was shared. Powerful personal experiences of supporting palliative care development and medical student education in Gaza were outlined, concluding with one student’s description of palliative care as ‘humanity until infinity’.
Dr Yasser Abu Jamieh (Gaza and Italy) presented ‘Gaza Community Mental Health programme. Rethinking trauma and healing’. A reminder of the challenges experienced in Gaza prior to October 2023, was shared, with the impact of the subsequent conflict including widespread destruction of infrastructure and multiple displacements of people. Powerful children’s art therapy was presented, demonstrating the internal and external impacts of the war, highlighting the magnitude of internal pain experienced. The ongoing impact of collective trauma, in both adults and children, was outlined, and the strength of community and family support emphasised. The critical importance of mental health interventions during crisis and trauma was outlined, especially pertinent in Gaza due to the relentless impact of multiple traumas from ongoing conflict. The session concluded emphasising the equality of all people.
Rev Rick Bauer’s (USA and East Africa) session focused on integrating spiritual and existential care in the midst of conflict and trauma. Participants were challenged to consider how they can support people dealing with loss and grief in situations of unimaginable devastation, with the importance of listening to, being alongside and not running away from, people experiencing spiritual distress in conflict and trauma being subsequently emphasised. Healthcare workers were also reminded to both recognise, and value, their own humanity as much as their clinical skills. The relatively new field of disaster spiritual care was shared, with the challenges of how to create space for prayer and ritual in the midst of disaster, in addition to providing a source of hope, being discussed.
The second part of the morning session comprised a series of short online recorded interviews with doctors sharing their experiences of working in conflict zones. Prof Khamis Elessi (Gaza and Jordan) was interviewed by Dr Mhoira Leng and stressed that humanity is a critical component of the healthcare role, to subsequently enable appreciation of the suffering experienced by others. He reminded participants of the obligations we have to care for all people, wherever they are, and to maintain hope for a better future.
Dr Nahla Gafer (Sudan and Egypt) was also interviewed by Dr Mhoira Leng and shared her personal journey of displacement in Sudan during the conflict, in addition to her work in cancer and palliative care. Her learning from both these experiences included the importance of information giving, communication and connection with family and colleagues.
Dr Olena Riga (Ukraine) was interviewed by Joan Marston (South Africa) and outlined the importance of developing an action plan for palliative care in conflict, prior to the event. She also shared how she derives hope and energy from patients and their families, in addition to collaborations with local and international colleagues.
Discussions, both in-person and online reflected on the powerful sessions and considered individual response. Areas addressed included the importance of locally led, contextual palliative care programmes being integrated in primary care systems and emergency response, and the importance of humanity and compassion on both a local and global scale.
The afternoon session was purely in-person and comprised a series of short presentations, interspersed with discussion.
Dr Anna Cleminson’s (Ireland) presentation focused on palliative care education in conflict, sharing experiences from Gaza. The importance of joint working between local and international colleagues and the two-way learning that took place was emphasised. The need for trauma sensitive crisis support was highlighted, in addition to supporting sustainable education approaches that were appropriate to the conflict setting.
Dr. Nuhamin Gebre (Ethiopia) gave an overview of her PhD research, exploring digital health in palliative care. The development, testing and launch of a mobile App in Ethiopia was outlined, with conference participants expressing interest in learning more about the App and potential transferability to a UK setting. Dr Gebre also emphasised the importance of empowering community health workers in Ethiopia.
Further discussion included an update on current bereavement research in Africa, with a focus on empowering communities to support in loss. The traumatic impact of both uncertainty and grieving when there is no actual body present to mourn, in conflict settings, was also considered. Additionally, the importance of helping people remember through silence and ceremony, and the question of how to incorporate ritual into individual and collective bereavement was also deliberated.
The conference concluded with a reminder of both the value of our collective humanity and compassion, and of the need for healthcare workers in situations of conflict and trauma to ensure they care for their own soul/spirit to enable them to continue in their work.
Thank you again to Michelle for sharing this excellent report with us, and for all her hard work in organising the conference, as well as the rest of the organising committee. We hope you have picked up a flavour of the topics and discussions and will join us for future conferences. Video recordings of the morning plenaries will be available soon on our website, keep an eye on social media channels and our newsletter for more info.
Conference Poster

Prof Liz Grant welcoming attendants to the conference
Rev Rick Bauer delivering a talk on integrating spiritual care into palliative care
Dr Mhoira Leng speaking on palliative care in humanitarian emergencies

Some of the attendants at the Roundtable discussion