
End of Year Reflections and Ways to Give
![]() Hannah Ikong
Hannah Ikong
![]() 16th November 2022
16th November 2022
For almost two decades, Cairdeas has endeavoured to support quality, accessible palliative care in resource-limited areas around the world. Cairdeas began with friends and colleagues in 2005 and soon grew to hold a mutual vision to work alongside existing and emerging palliative care services:
- supporting education, training and curriculum development
- offering specific clinical expertise, such as mentoring and service design
- and, raising the profile of palliative care needs.
A Scottish Gaelic word, “Cairdeas” means worldwide friendship, and in this year of 2022 we couldn’t agree more. Our friends, colleagues, individual and organisational partners throughout the globe are foundational to our vision where palliative care is accessible by all.
We thank you for your giving of time, talents, and resources over the years. From the recent difficulties of navigating the COVID-19 pandemic to the milestones of beginning the Cairdeas mission, expanding to places like India, Uganda, the Sahara and Gaza, we have been grateful to walk step by step alongside you.
We also celebrate our achievements together in providing excellent palliative care for all. From our early years of mutual growth of Pallium India and Christian Medical College, Vellore, to the leadership development of a new palliative care unit in Mulago Hospital and Makerere University in Kampala, Uganda (MPCU), we are honoured and proud of the progress we have made together.
This year, as MPCU makes 14 years of service and now operates in both Mulago and Kiruddu Hospitals, we are also partnering with the Islamic University in Gaza to establish a diploma programme for palliative care. (More information to come!)
We are thankful for what we have accomplished together and are eager to see what the next years have in store. We invite you to draw close and interact in this journey of quality palliative care for all, as we suggest the following:
Stay connected to new happenings. You can register to be notified of new blogs or follow our social media pages on Facebook and Twitter.
Purchase picturesque calendars. For those in the UK only – limited time only – Stewart Kerr has offered beautiful sceneries of Scotland, with all proceeds going to Cairdeas.
Stewart shared:
I am fundraising again this year for Cairdeas International Palliative Care Trust with a new Scottish landscape calendar for 2023. The format is the same as last year. They are A3 in size (297 x 420 mm) on 250gsm coated stock. They are available at £14 each plus £2.50 UK postage if required (plus any additional donation you care to make) with ALL money going to Cairdeas.
If you would like to order any, please just get in touch either directly or using the email below letting me know how many you would like and an address if you would like them posted … Email: calendars@stewartkerr.com
Shop online and give to Cairdeas. Register on Amazon Smile, Give as You Live, or Easy Fundraising, where a percentage of your online purchases will automatically be donated to us.
Consider volunteering with partners, PallCHASE or PcERC. Simply send a quick email to our global partner PallCHASE (Palliative Care in Humanitarian Aid Situations and Emergencies) or to PcERC (Palliative care Education and Research Consortium) in Kampala, Uganda.
Donate for long-lasting impact. Giving at Cairdeas goes towards building capacity for village health teams and healthcare workers, or you can contribute towards the Cairdeas Scholarships programme to sponsor a year-long diploma or three-year degree in palliative medicine. You can donate to Cairdeas directly or give to PcERC’s Global Giving page.
Thank you for extending worldwide friendship and fellowship, Cairdeas, to the areas that need palliative care services the most. With each patient and family provided with holistic care and with every healthcare worker trained, we advance the mission to promote and facilitate the provision of high-quality palliative care to all.

Cairdeas: Worldwide friendship or fellowship.

The “Hats on for Children’s Palliative Care” day of 14th October coincided with the Palliative Care Conference at the Sri Guru Ram Das University of Health Sciences, Amritsar, India.

The MPCU / PcERC team fills the frame at their Clinical Office 4B at Mulago Hospital.
Sneak preview of the 2023 Calendar for Cairdeas fundraiser … make your order today!

Current Cairdeas Scholar Phillip Amol Kuol gives a quick smile after taking a call from his mother in South Sudan. Phillip is studying social work and social administration and serves in a Village Health Team (VHT) in Adjumani, Uganda.

As our year comes to an end, another one begins … let us enter 2023 together.
World Hospice and Palliative Care Day in Kampala, Uganda
![]() Hannah Ikong
Hannah Ikong
![]() 10th November 2022
10th November 2022
With twenty-nine years of palliative care services in Uganda, World Hospice and Palliative Care Day (and the week leading up to it) was something to celebrate.
One notable event was a public lecture on palliative care, which was organised by the Ministry of Health (MOH) plus the Palliative Care Association of Uganda (PCAU) and facilitated at the Davis Lecture Hall (Makerere College of Health Sciences, Mulago Hospital). It was encouraging to see so many students and healthcare professionals, as well as the online attendees on Zoom, on the afternoon of Wednesday, 5th October.
The team of Mulago Palliative Care Unit (MPCU)/Palliative care Education and Research Consortium (PcERC) was actively engaged in the public lecture. The team managed the registration table and handed out brochures and drinks. Both the team working in Kiruddu and Mulago Hospitals came for the event and were very proud to see their own Dr Liz Namukwaya present about the unit and sit in the Q&A panel.
Dr Liz Namukwaya spoke on the unit’s clinical activities, role in education, and extent of research. With an estimated 46% of patients admitted needing palliative care, the palliative unit alongside LINK nurses has served 12,520 patients since 2008. The unit has also trained over 3,500 students, from postgraduate and undergraduate doctors, nurses, pharmacists, to social workers.
Several other doctors presented on palliative care; first, Dr Fredrick Nelson Nakwagala, the Clinical Head Directorate of Internal Medicine at Mulago Hospital, talked about non-malignant conditions requiring palliative care. He shared stories of breaking bad news and encouraged fellow healthcare professionals to see the patient as a person, not as their illness. Dr Peter Lwabi, the Deputy Executive Director of the Uganda Heart Institute, then addressed the interdisciplinary approach of palliative care and cardiology.
The keynote speaker Dr David Okello presented on community engagement for alleviating pain and suffering in palliative care patients. As the Executive Director at African Center for Global Health and Social Transformation, he shared about the effectiveness of community involvement in COVID-19 and how the community contributes to holistic care.
The public lecture availed to much discussion among the Q&A panel and several remarks from palliative care leaders in attendance. The questions from the audience had to be cut short due to time, yet many were requesting for palliative care refresher trainings. Dr Anne Merriman, founder of Hospice Africa Uganda (HAU), gave some of the closing remarks as she reminded us to take care of the carers; that is, amid all the clinical activities, training, and research, we ought to care for ourselves and our colleagues.
World Hospice and Palliative Care Day (WHPCD) then was on Saturday, 8th October. The theme for this year was “Healing Hearts & Communities” which aligned well to the messages shared in the public lecture.
The palliative care unit of MPCU/PCERC was actively involved in the day’s events from the National Palliative Care Walk in the morning to the PCAU Palliative Care Fraternity football match. The unit contributed to the sponsorship of the day and assisted with the organisation, and they were glad to meet others who worked in palliative care across Uganda. The walk was about 4 km long, which started in the Mulago field/playground to Kamwokya (around Acacia Mall) and back again.
Liz Nabirye, the Clinical Lead of PcERC, noted that “it was a good health exercise and the first time to celebrate together since COVID. Later back at Mulago, we had speeches were made from the director of PCAU [Mark Mwesiga] and each palliative care organisation had time to talk about what they do.” She specifically recalls meeting other units from Masaka in western Uganda as well as Jinja (east-central), and they were able to share what services they offer and how they could refer patients to each other. “It was a unifying celebration for us, it was a palliative care fraternity,” Liz concluded.
This day of advocacy and awareness to palliative care was true to its theme, and healing hearts and the community involved a bit of fun! The team had practiced for weeks for this, and how it was finally here: a football match of representatives of the palliative care fraternity against members of the Ugandan Parliament. The two representatives from PcERC, Toko Friday and Bemustar, played well and tried their best. But in the end the parliamentarians wone the match, 6-3.
Nevertheless, PcERC was awarded a certificate of participation, and the team brought many good memories and new contacts from the day. “For me as the lead,” Liz Nabirye told me, “I would just say being a part of the events was a good thing to happen to our unit; we were able to create awareness, be represented, and be involved in the preparations. The week was for our advocacy … it raised visibility for palliative care services at the national referral hospitals.”

The official advertisement for the World Hospice & Palliative Care Public Lecture hosted by the Ministry of Health and the Palliative Care Association of Uganda.

A member of the audience inquiries the panel about how to encourage colleagues in their treatment of patients suffering and in pain.

The panel in person and on Zoom; questions kept coming in from both audiences! Pictured from left to right: Dr David Okello, Dr Fredrick Nelson Nakwagala, Dr Liz Namukwaya, and Dr Peter Lwabi.

Final remarks from Dr Anne Merriman of Hospice Africa Uganda: “Care for the carers.”
Official invitation to the walk sponsored by the Ministry of Health and the Palliative Care Association of Uganda.

The team from PcERC watching the football match; left to right, Liz Nabirye, Josephine Kabahweza, Vicky Jeminah, and Ronald Mukasa.

Our football player Toko Friday Santiago takes a quick break and stands near the team.

The certificate of participation to PcERC for World Hospice and Palliative Care Day and Week.
Photovoice and Palliative Care: Expanding Research in Adjumani and Obongi
![]() Hannah Ikong
Hannah Ikong
![]() 10th November 2022
10th November 2022
We are eager to incorporate Photovoice into the Transform Project in the Adjumani and Obongi districts of Uganda. Photovoice adds a deeper layer to the current data collection, helping us to better understand the lived experiences of severe health-related suffering (SHS) whilst staying in fragile communities. Photovoice is rather new in palliative care research in Africa, but on 22nd August we were able to receive a refresher training from Dr Jane Bates who utilised Photovoice with patients and their families and caregivers in Malawi.
What is Photovoice exactly? Perhaps we can first tell you what it is not: Photovoice is not when a medical researcher visits a new area, evaluates a patient while taking pictures of the setting, then shares a story of what they found. Rather Photovoice is a dialogue where the patients (and/or families and caregivers) use photography to express themselves and share what is most important to them. Photovoice is a great addition to advocacy and self-representation, for it allows the community to speak for themselves by removing the newcomer’s perspective in the storytelling. Dr Jane Bates includes the three goals of Photovoice in her article, Enhanced patient research participation: a Photovoice study in Blantyre Malawi:
1. To enable people to record and reflect their communities’ strengths and concerns.
2. To promote critical dialogue and knowledge about important issues through large and small group discussion of photographs.
3. To reach policymakers.
During the refresher training, Dr Jane Bates spoke about her experiences of using Photovoice among patients with palliative care needs and their families and caregivers. As palliative care, in itself, has a patient-centred approach, it was thought best to use this participatory method of research, allowing those being ‘researched’ in Malawi to become the ‘researcher.’ Conducting the study at a community-based palliative clinic, they recruited six patients and seven carers as co-researchers during a period of four months. Their co-researchers were given digital cameras and through some nine group sessions, they took pictures, selected, and analysed their printed photos, later captioning a few of them in their own words. This process was reported to aid in open dialogue and, at times, assist in clinical review. The third goal of reaching policymakers through Photovoice was achieved at the end of study when they held a photo exhibition and advocacy event, which was attended by the local leaders and media.
Dr Jane Bates also discussed some cautions or concerns raised from their Photovoice study. For instance, this method of research excluded some patients with severe palliative care needs who could either not attend the sessions or see the pictures well. For others who were able to work, the structure of the group meetings was a challenge and they ended up missing some sessions as they needed to work and provide for themselves.
She challenged the leaders of the Transform Project to consider how we could bring Photovoice to Adjamani and Obongi districts, and how we could accommodate those who are more seriously ill and those who need time to work and make a livelihood. We then discussed our proposed research structure that may mitigate these challenges. For one, the trained Village Health Team members (VHTs) carry a smartphone with a camera, so they would work with the patients and their families individually to take photos, select and analyse them. VHTs also do travel to a patient’s home, giving those who are immobile an opportunity to participate and have a voice. Ideally, our VHTs could also liaise with those who are working outside the home and find times to meet and share in the Photovoice research.
It is clear to the Transform Project leaders that Photovoice is a necessary addition in our data collection. We already have the backbone needed for this participatory research method; the VHTs hold smartphones and have been trained how to use the camera, we have a network of patients, families and other caregivers visited regularly by the VHTs, and now our leadership team has been trained in Photovoice methods and the process. The next step will be sharing what we have learned with the VHTs so they can begin the Photovoice process.
Liz Nabirye, clinical lead of PcERC and a part of the Transform leadership found the training applicable to more than just our research in Adjumani and Obongi districts. “To me,” she said, “it is not just a methodology to use for this project, but to train our volunteers in the Kampala Hospitals to learn to use Photovoice and engage with our patients and our families. Photovoice is a strong method of getting quality, important information … [we can] work with the patients and their families and make meaning of the photos and what they are communicating to us.” We thank Dr Jane Bates for the invaluable mentorship she has given the team by sharing her own experiences and advising us in integrating Photovoice to our current research. Do stay tuned for more Photovoice updates, coming soon from Uganda!

Transform Project leaders pose for a photo with Dr Jane Bates. Pictured from left to right: Dr Mhoira Leng, Toko Friday Santiago, Immaculate Atim, Dr Jane Bates, Liz Nabirye, Dr Liz Namukwaya, and Godfrey Oziti.

Selfie time with the author of this blog, Hannah Ikong.
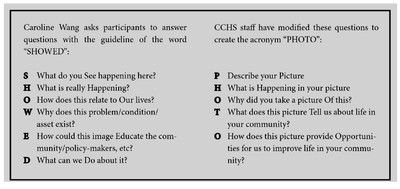
Discussion questions for Photovoice dialogue shared by Dr Jane Bates. We walked through each question and even participated in role plays to see how “SHOWED” and “PHOTO” questions could facilitate deeper discussions.